The risks of diagnostic errors in all care settings

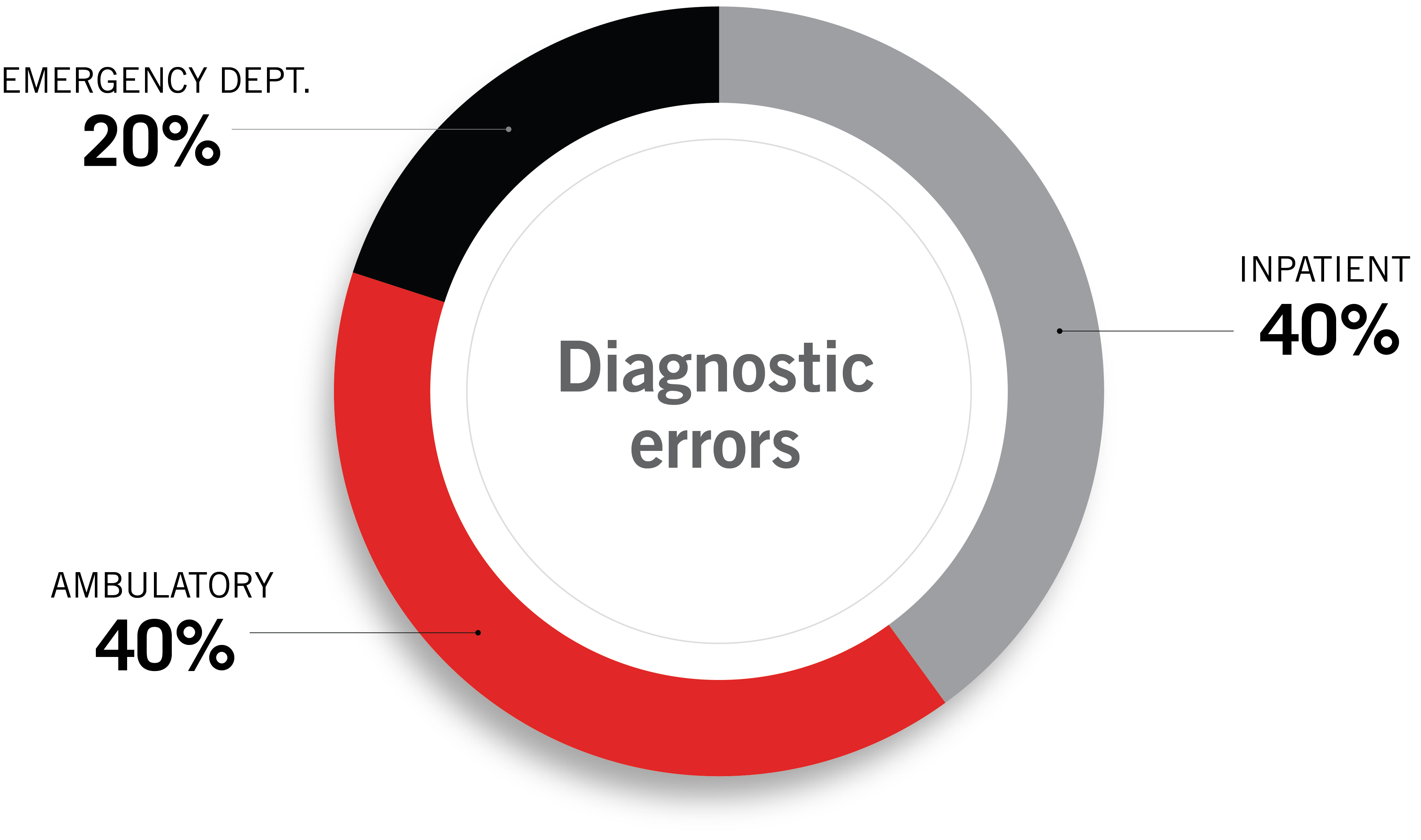
Dana Siegal | Vice President, Risk Management and Analytics, Coverys Medical patients do not expect healthcare providers to make diagnostic errors, no matter where they seek care. Until recently, clinicians and others believed most diagnostic medical errors occurred in ambulatory settings, including the emergency department (ED). Deeper research, however, shows the components of diagnostic errors impact care regardless of the setting. In fact, the occurrence is equally distributed across inpatient and ambulatory settings. Why is this the case, and how can the healthcare industry address it? The data leads us to ask two key questions about the diagnostic process: Clinicians need to make numerous decisions every day based on the information they have on patients in their care. Coverys claims data has found while some elements of diagnostic errors are similar across the continuum, there are some key differences in different settings: Diagnostic needs in the ED are generally focused on the primary diagnosis of a new injury and/or the evolution of new onset symptoms in a chronic or newly developing clinical condition. The acute nature of the diagnostic need requires rapid assessment and decision-making and readily available test resources, results, and consulting. It can be hindered by lack of clear medical history and description of the current scenario, e.g., an unconscious patient, poor historian, lack of prior medical record, or input from previous providers or family. Additional error-enabling factors include the often-hectic environment of the ED; timeliness of needed resources such as lab, radiology, or consultation; as well as communication and processing of all that information and the impact of clinical judgment biases. These include, for example, narrow diagnostic focus and anchoring or confirmation bias resulting in premature discharge. Issues involving pending test results at discharge or follow-up on edited radiology results add an additional level of complexity in ED care by creating the potential for critical communication gaps with the patient. For ED patients who get admitted to inpatient care for continued exploration of the primary diagnosis, there may also be additional elements of anchoring on concurrent diagnosis differentials established in the ED as well as communication and handoff issues. For example, when a patient transfers to inpatient care, information sharing and documentation are essential. What was the primary diagnosis in the ED? What test results are still pending? Inadequate or missing documentation can result in lack of critical information by the inpatient care team. While ambulatory care may well be impacted by the same information gathering, assessment, and processing issues as the ED, there are additional system complexities in the ambulatory setting that can result in delays in getting to the right diagnosis and/or communicating that to the patient. There may be days and often weeks between visits, access to consultations and advanced testing may be delayed, and patients may not choose or be able to follow up with scheduled/recommended tests, and the potential for loss of continuing communication grows with the timeline and number of providers involved. Quite often, the diagnostic error or failure is not of the primary diagnosis but of a complication of current medical or surgical care. One common area of this is postoperative and postprocedural care. Whether inpatient or ambulatory, postoperative and postprocedural complications have elements of both ED and ambulatory care vulnerabilities. Medical complications arise following surgeries and other procedures, and this is where the critical skills of clinical monitoring come into play. Whether inpatient or surgical, monitoring and communicating the often-subtle signs of evolving complications immediately postop/postprocedure are critical skills to diagnose such acute complications as hemorrhage or cardiac decline. Failure to recognize and/or communicate these concerns can result in actions delayed or not taken and the sudden deterioration of the patient’s condition. If discharged before such complications are fully evaluated and for complications that may take longer to declare themselves, such as an evolving pulmonary embolism or infection/sepsis, the ambulatory setting adds additional complexities for patients and families trying to determine if/when/how to best communicate these concerns when they evolve at home. Additionally, providers and their care teams are often confronted with the need to “triage” such concerns virtually (e.g., calls, portal communication) balancing the need to assure patients of the “normal” expectations while processing the clinical picture and assessing the need for immediate follow-up care. A critical step in mitigating the risks of medical errors is to identify and understand their root causes. Providers and healthcare facilities need to leverage and analyze their data and be inquisitive as to the vulnerabilities and errors they discover in these reviews. When a diagnostic error does occur, healthcare professionals need to understand what happened and take steps to prevent it from recurring. Here are three key areas of focus for improving risk control in diagnostic errors: Education and engagement. We cannot fix or improve what we don’t recognize or understand. Healthcare organizations need to embrace opportunities to educate those who deliver direct care to patients on the risks and vulnerabilities that cause diagnostic error and harm. Adverse events (and near misses), quality metrics, case and peer reviews, and medical malpractice analysis all provide critical insights that can help caregivers on the front lines understand the drivers of error and harm in their practices for safer care and better outcomes. Equally important, these data points validate the actual improvement needs, supporting leadership in prioritizing the time and resources to address these critical risk and patient safety needs. Diagnostic timeouts in the ED, discharge huddles in ambulatory surgery and procedure settings, and accountability to monitoring and escalation in the inpatient settings are all ways in which a team can connect, share, and collaborate on processing the critical information required for maximum diagnostic safety and excellence. Creating a culture with clear expectations of and adherence to best practices, providing safe, non-punitive avenues for sharing concerns and errors, and addressing missteps and deviations in a fair and just process, are the very foundations of a culture of safety for patients, staff, and providers. To ensure maximum success, it is critical that leadership promote and actively support their commitment to safety. Staff should feel safe, heard, and validated when they raise concerns. And providers need to be embraced and engaged as part of the risk, quality, and patient safety spectrum of process improvement. To sustain such a culture across all care settings is the best and only way to build a legacy of diagnostic excellence for your entire organization. Diagnostic errors remain a significant problem in the U.S. healthcare system and are a key source of malpractice claims. A study published in July 2023 by a research team led by the Johns Hopkins University School of Medicine and supported by others (including myself, Dana Siegal, as one of the research team members) estimated 795,000 Americans die or are permanently disabled each year due to misdiagnosis, across care settings. Healthcare organizations can combat this serious problem through concerted efforts to improve patient safety, increase accountability, and ensure commitment to delivering the safest care possible, regardless of setting. For more information on tools and strategies to assist with risk management in healthcare, please visit www.coverys.com. Coverys insurance products issued by Medical Professional Mutual Insurance Company and its insurance subsidiaries, Boston, MA. This article is for informational purposes only and may not reflect the most current legal or medical developments. This informational material is not intended, and must not be taken, as legal or medical advice on any particular set of facts or circumstances.
Types and complexity of diagnostic exposures
Mitigating risks of misdiagnosis
 Dana Siegal is Vice President, Risk Management and Analytics, at Coverys, an innovative provider of medical malpractice insurance dedicated to helping policyholders anticipate, identify, and manage risks to reduce errors and improve outcomes. During her extensive career, Siegal, a registered nurse, has served as Director of Patient Safety at CRICO Candello and on the Board of Directors for the Society to Improve Diagnostic Medicine (SIDM).
Dana Siegal is Vice President, Risk Management and Analytics, at Coverys, an innovative provider of medical malpractice insurance dedicated to helping policyholders anticipate, identify, and manage risks to reduce errors and improve outcomes. During her extensive career, Siegal, a registered nurse, has served as Director of Patient Safety at CRICO Candello and on the Board of Directors for the Society to Improve Diagnostic Medicine (SIDM).
Lorem ipsum dolor sit amet, consectetur adipisicing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut.
Lorem ipsum dolor sit amet, consectetur adipisicing, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut. Ut ad minim veniam.
Vestibulum ante ipsum primis in faucibus orci luctus etel ultrices posuere cubilia Curae.
Lorem ipsum dolor sit amet, consectetur adipisicing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut.
Sed ut perspiciatis unde omnis iste natus error sit voluptatem!
Nemo enim ipsam voluptatem quia voluptas sit odit aut fugit!
Ut enim ad minima veniam, quis nostrum exercitationem ullam!

"Et harum quidem rerum facilis est et expedita distinctio!"

"Nam libero tempore, cum soluta nobis est eligendi."

"Temporibus autem quibusdam et aut officiis debitis!"